In the world of MedTech R&D, there is a recurring point of friction that stalls innovation: the “Static-to-Dynamic Gap.”
Medical imaging has advanced tremendously. We can take high-resolution MRI or CT scans and convert them into incredibly detailed 3D reconstructions. However, for intra-operative guidance and advanced surgical training, static 3D files (like STLs) or pre-rendered MP4 animations are insufficient.
Surgeons struggle to correlate a static 3D model viewed on a desktop with the dynamic, restricted, and continuously shifting environment they experience through an endoscope or laparoscope.
To build tools that actually improve clinical outcomes, we must transform static data into interactive, real-time simulations.
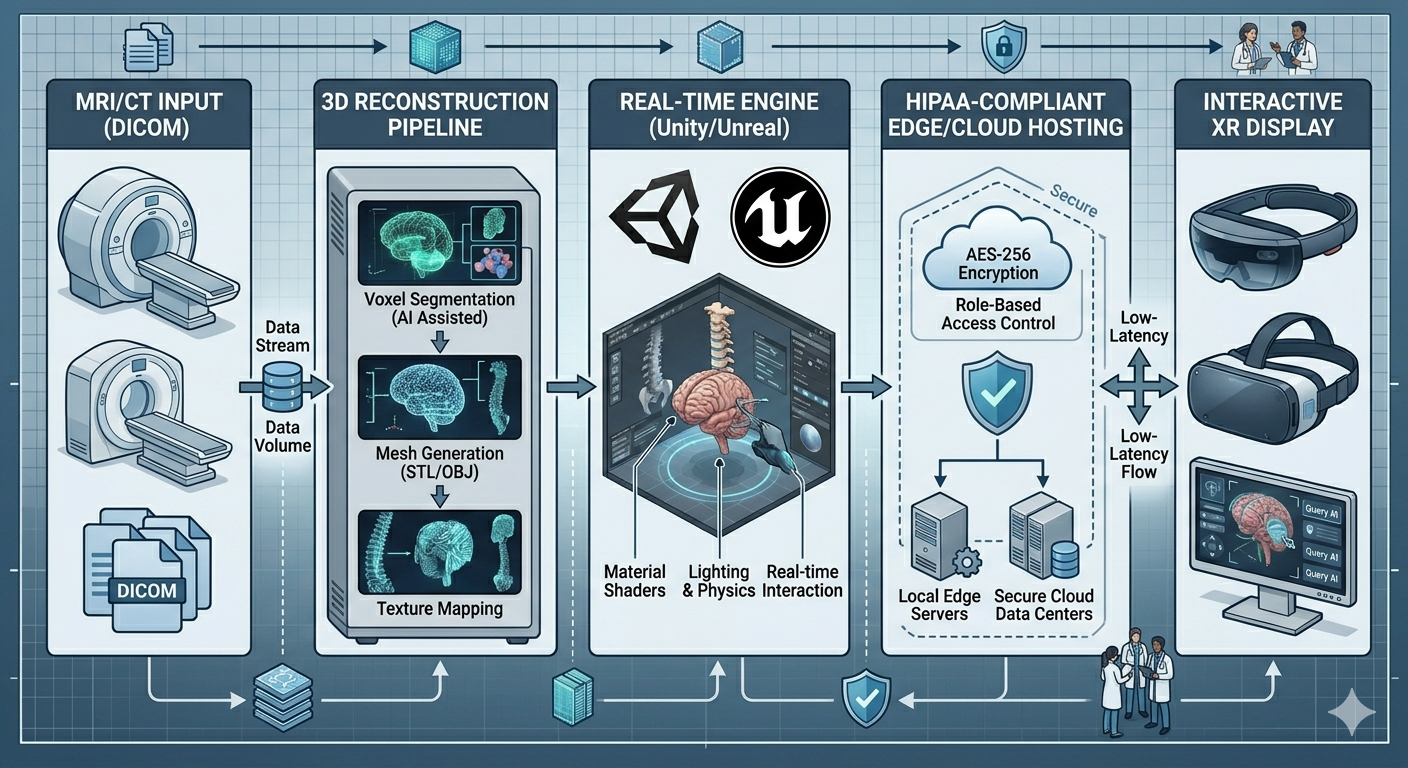
The Strategic Shift: From Pre-Rendered to Real-Time The architectural solution requires moving away from traditional rendering software and adopting Real-Time 3D Engines (such as Unity URP or Unreal Engine) as the core visualization layer.
By establishing a real-time engine architecture, we unlock capabilities that are otherwise impossible:
Low-Latency Interactivity: We can simulate a virtual laparoscope with 6 Degrees of Freedom (DOF), providing the tactile-visual feedback necessary for surgeons to build spatial muscle memory. Dynamic Occlusion & Lighting: We can programmatically simulate the harsh lighting and deep shadows of the abdominal cavity, reacting in real-time as the virtual camera moves. Algorithmic Highlighting: By utilizing custom rendering shaders, the architecture can ingest metadata from an AI diagnostic model and dynamically highlight specific pathologies (e.g., making a tumor margin emit a distinct visual glow under simulated lighting conditions).
Architecting for Surgical Constraints A major bias in early-stage surgical simulation is “perfect omniscience”—giving the user a perfectly lit, 360-degree view of the anatomy. This is not reality.
A true surgical architecture must simulate physical limitations. For example, a laparoscope has a highly restricted field-of-view (FOV). The architecture must incorporate dynamic UI masking and camera constraints to force the simulation to match the exact optical reality the surgeon will face. This ensures that the AI guidance tools being developed are tested under realistic conditions.
Article content The Infrastructure: Compliance Meets Performance Rendering these environments in real-time requires immense computational power. However, because this data is inherently derived from patient scans (PHI), it cannot simply be processed on public, unsecured servers.
The architectural best practice is to deploy secure, HIPAA-compliant GPU-enabled Virtual Machines (e.g., utilizing localized AWS, GCP, or Azure instances with strict data sovereignty protocols). This ensures that heavy rendering happens off-device, enabling cross-platform streaming to XR headsets or web browsers without ever exposing the underlying patient data to unauthorized endpoints.
The ROI of Real-Time Architecture For a MedTech executive, establishing this pipeline is not just about better graphics; it is about R&D velocity. By creating an architecture that can instantly ingest patient-specific data into a navigable simulation, you drastically reduce prototyping time, standardize surgical training, and prove the efficacy of your visual intelligence tools before stepping foot in an actual operating room.
Successful surgical simulation requires a specific bridge between medical data and game-engine performance. I have documented the core principles in a 1-page guide: ‘Architectural Best Practices for Real-Time Surgical Simulation’.
Comment “BLUEPRINT” on my LinkedIn post, and I will DM it to you directly.