Over the last 11 articles, we have systematically deconstructed the architectural bottlenecks that plague MedTech and Healthcare AI.
We moved from the foundational logic of structuring unstructured clinical text via LLMs and RAG, to the optical constraints of deploying sub-20ms Computer Vision at the surgical edge. We then bridged those domains, projecting this intelligence into the surgeon’s field of view through Augmented Reality and Vision-Language Models (VLMs).
If you have followed this journey, one reality should now be abundantly clear:
Building clinical-grade AI is not a software engineering problem. It is a systems architecture problem.
The Silo Trap: Why MedTech Innovation Stalls In my capacity as an architect consulting for surgical robotics and digital health firms, I repeatedly encounter the same organizational friction.
A company will have a brilliant data science team building highly accurate CNNs for pathology. Down the hall, a separate team of 3D engineers is building Unity-based surgical simulations. Meanwhile, the IT compliance team is isolated, trying to figure out how to bolt HIPAA security onto the resulting products as an afterthought.
When these systems finally meet in integration testing, the latency spikes, the spatial registration drifts, and the clinical context is lost. The product stalls in “pilot purgatory.”
You cannot bolt these technologies together. They must be orchestrated from the ground up by a unifying architectural vision.
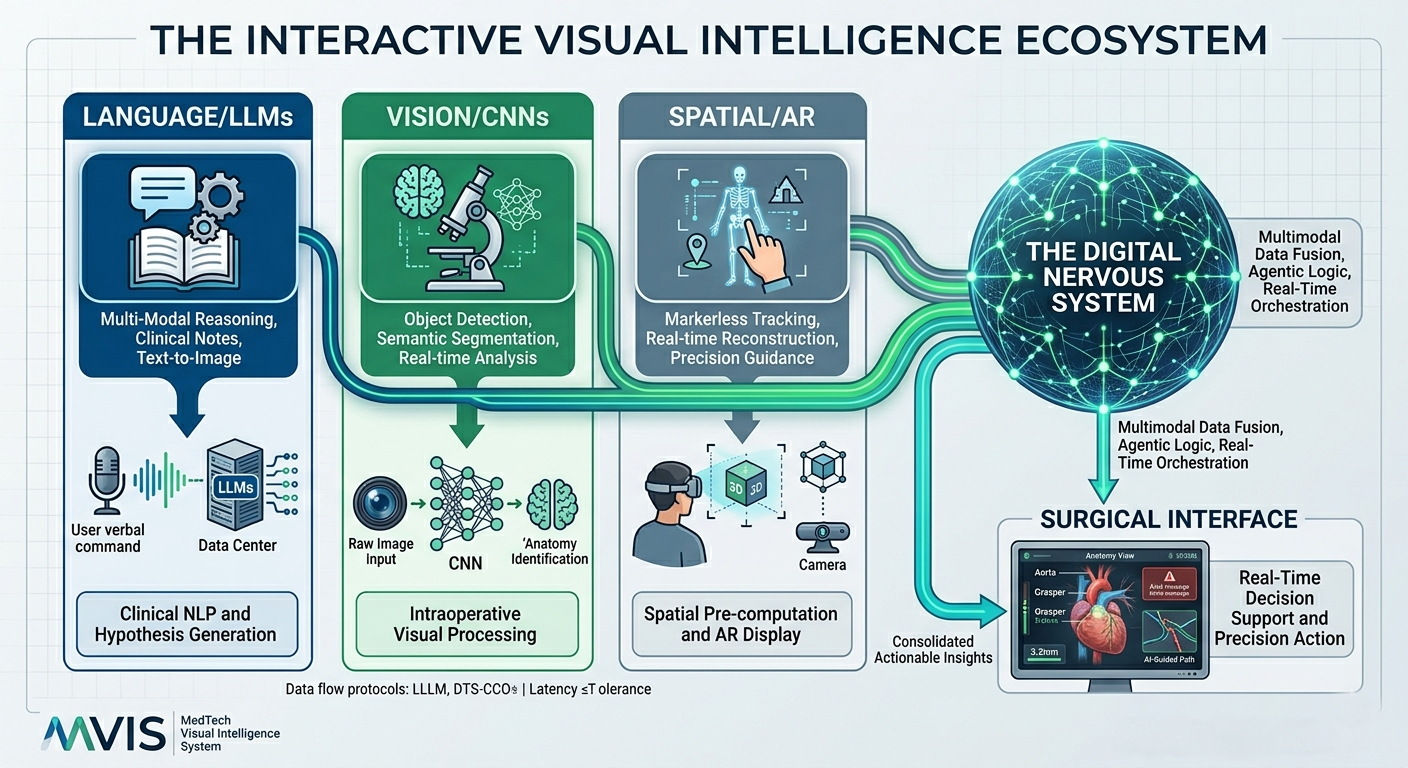
The Interactive Digital Nervous System The future of MedTech belongs to the organizations that can build an Interactive Digital Nervous System. This requires a paradigm shift:
Holistic Infrastructure: Edge-GPUs, zero-hallucination vector databases, and real-time rendering pipelines must be treated as a single, interdependent organism. Multimodal by Default: A surgeon shouldn’t have to look at a monitor for a classification, check a tablet for a patient history, and use a separate AR headset for navigation. The architecture must natively support VLMs that can “see” the anatomy and “speak” the clinical context simultaneously. Clinical Constraints as Code: Latency limits (sub-20ms), field-of-view restrictions, and spatial occlusion are not bugs to be fixed later; they are the foundational constraints upon which the code must be written.
How We Architect It Together (The Pitch) This level of orchestration requires a highly specialized blend of academic rigor and agile, real-world deployment experience.
At IIT Bombay, I mastered the first-principles mathematics that govern applied algorithms. Over the next decade, from building complex spatial engines to architecting precision surgical AR systems, I learned how to deploy that math in the most uncompromising, high-stakes environments on earth.
I do not just write code; I design the blueprint that ensures your engineering teams build the right code.
As a Fractional CTO and Strategic Technical Architect, I partner with MedTech innovators, Chief Medical Officers, and VPs of Engineering to:
Audit and unblock stalled surgical AI and AR pipelines. Design end-to-end architectures for zero-latency, compliant visual intelligence. Train and elevate internal engineering teams to execute at the intersection of AI, CV, and Spatial Computing.
Article content