We are officially entering Phase 2 of this series. For the last two weeks, we explored how to extract intelligence from unstructured clinical text using LLMs. But the operating room (OR) presents a vastly different challenge. The OR is highly dynamic, visually chaotic, and completely unforgiving of delays.
In a recent comment on my first article, a clinical data analyst made a profound point: “Decision analytics in clinical settings needs to be both fast and reliable. Even small delays or inaccuracies can affect outcomes, which makes system design extremely important.”
Nowhere is this more critical than in Laparoscopic Computer Vision.
Minimally invasive surgery restricts the surgeon’s field of view to a 2D monitor and eliminates direct tactile feedback. They rely 100% on the optical feed. When MedTech innovators attempt to augment this feed with Artificial Intelligence—highlighting unseen tumors, mapping the biliary tree, or identifying critical blood vessels to prevent accidental severing—they immediately encounter the hardest architectural challenge in spatial computing: The Latency Trap.
The Physical Reality of the Operating Room In my years architecting mixed reality and vision systems, transitioning from standard commercial environments to surgical environments requires a fundamental unlearning of standard software architecture.
If a cloud-based chatbot takes 2 seconds to generate a response, the user waits. If a surgical augmented reality overlay takes 200 milliseconds to render a bounding box around an artery, the surgeon’s scalpel has already moved.
When visual feedback lags behind proprioceptive (physical) movement, it induces “simulator sickness” and spatial disorientation. The surgeon loses trust in the system, turns the AI off, and the multi-million dollar R&D investment gathers dust in the corner of the OR.
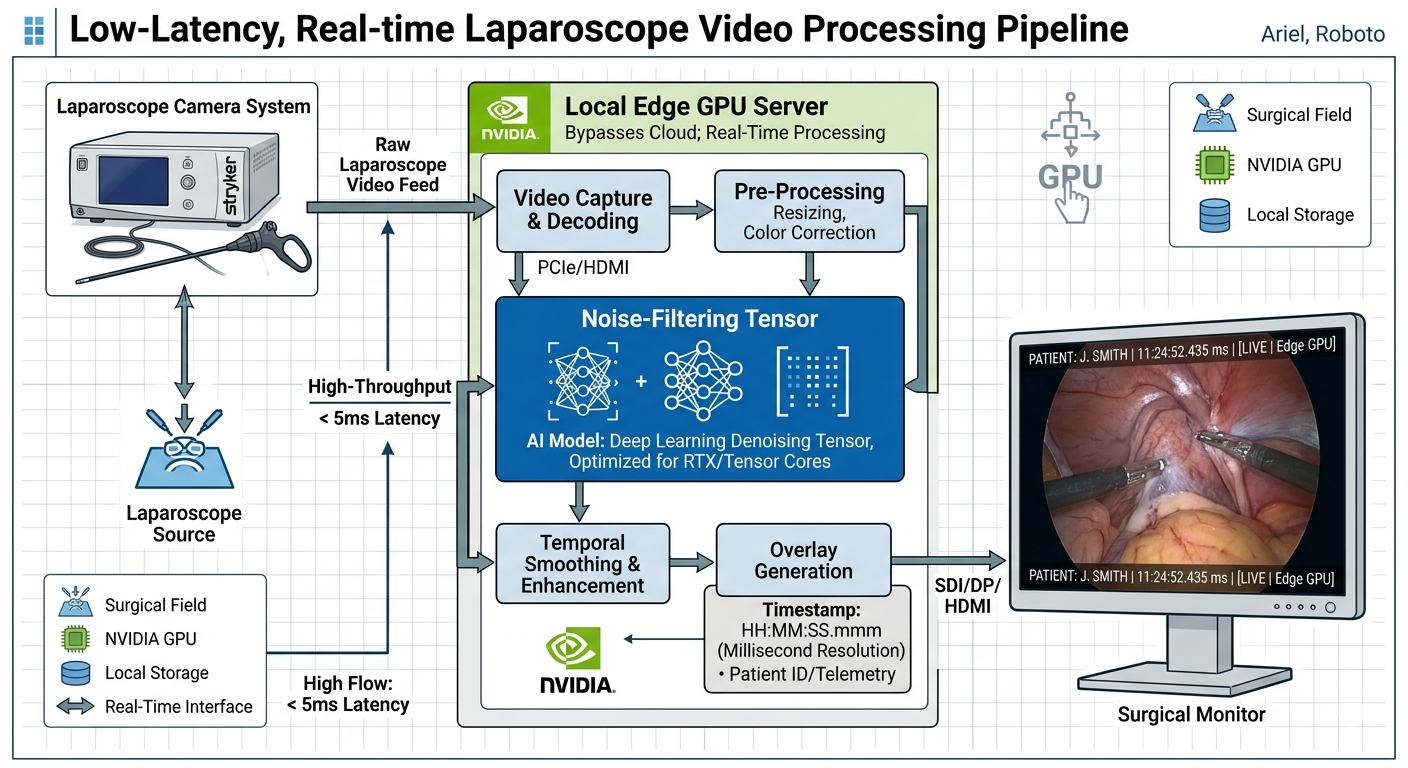
To be clinically viable, an intra-operative vision system must achieve “motion-to-photon” latency of less than 20 milliseconds.
Why Classical Edge Detection Fails in Surgery When prototyping these systems, engineering teams often start with classical computer vision techniques—the foundational math I studied deeply during my time at IIT Bombay. They attempt to use algorithms like the Canny Edge Detector to outline anatomical structures.
In a sterile, perfectly lit laboratory, these mathematical rules work flawlessly. In the human abdomen, they break immediately.
Surgical video feeds are uniquely noisy. They are plagued by:
Surgical Smoke: From electrocautery devices, which obscures the camera lens. Specular Highlights: Wet tissue reflects the harsh laparoscopic light source, creating blinding white spots that algorithms mistake for structural edges. Dynamic Deformation: Organs breathe, pulse, and shift when touched. Nothing is static.
If you rely on classical, rule-based edge detection, you are forced to constantly tune mathematical thresholds mid-surgery. The system will highlight the smoke instead of the tissue, blinding the surgeon.
The Architectural Pivot: Edge Computing and Learned Perception Article content To solve the Latency Trap and the noise problem, we must architect a system that abandons the cloud and abandons rigid mathematical rules.
-
Severing the Cloud (Compute at the Edge) Surgical Computer Vision cannot rely on AWS, Azure, or GCP for real-time inference. Hospital Wi-Fi is unreliable, and the round-trip data transfer guarantees unacceptable latency. The architecture must push the inference engine directly to the “Edge”—meaning deploying high-performance GPU hardware physically inside the surgical tower, hardwired to the endoscope.
-
From Rules to Representation (The Deep Learning Shift) Instead of writing fragile algorithms to detect edges, we must architect convolutional pipelines that learn to ignore the noise. By training neural networks specifically on noisy, smoke-filled surgical footage, the model learns the semantic difference between a glare on wet tissue and the actual margin of a tumor. (We will dive deep into architecting these Convolutional Neural Networks in next week’s article: Beyond the Human Eye).
The Executive ROI
Why does this matter to a MedTech executive? Because clinical evidence is finally catching up to technological capabilities. Health systems are no longer buying “cool AI.” They are buying systems that have proven, in rigorous clinical trials, to reduce complications like bile duct injuries or reduce surgeon cognitive load.
A system architected to beat the Latency Trap is a system that surgeons will actually use. And user adoption is the only metric that drives revenue.
Transitioning AI from the cloud to the surgical edge is a complex infrastructural challenge. I have mapped out the hardware and software topology for this in my 1-page guide: ‘Architecting Sub-20ms Edge Computing Pipelines for Surgical AR’.
Comment “BLUEPRINT” on my LinkedIn post, and I will DM it to you directly.
Conclusion
We are no longer limited by what the human eye can see through a laparoscope; we are limited only by our ability to process and render data in real-time.
If you are a CTO or Head of Innovation struggling to get your surgical computer vision prototype out of the lab and functioning reliably in the OR without lag, you have an architectural bottleneck. Send me a DM. Let’s schedule a strategic consultation to optimize your pipeline for the realities of the operating room.