Time is the most expensive commodity in medical research and technology development.
Whether your team is synthesizing literature for a new FDA 510(k) submission, investigating the efficacy of a novel surgical robotic tool, or performing pharmacovigilance, the bottleneck is rarely human intellect. The bottleneck is the sheer volume of fragmented, unstructured medical literature.
When you are paying top-tier PhDs, Chief Medical Officers, and R&D engineers to manually query PubMed, cross-reference clinical trial registries, and perform manual data extraction, you are misallocating your most valuable intellectual capital.
In Part 3 of this series, we discussed Retrieval-Augmented Generation (RAG). RAG is incredibly powerful, but architecturally, it is passive. It waits for a query, searches a pre-indexed internal database, and returns an answer. It acts as an elite librarian.
But to truly accelerate healthcare innovation, we don’t just need a librarian. We need an Autonomous Medical Researcher.
The Architectural Paradigm Shift: The ReAct Framework To achieve autonomy, we must shift our architecture from treating Large Language Models (LLMs) as mere text generators to treating them as Reasoning Engines.
This is accomplished through the ReAct (Reason + Act) framework.
During my foundational years studying Applied Algorithms at IIT Bombay, the focus was always on state-space search and deterministic logic flow. Over the last decade architecting scalable systems in the startup trenches, the challenge became marrying that deterministic logic with dynamic data. The ReAct framework does exactly this for modern AI.
Instead of outputting a final answer immediately, an AI Agent operates in a continuous, autonomous cognitive loop:
Thought: The LLM analyzes the user’s complex clinical query. It breaks the problem down. “I need to find the latest contraindications for Drug X, but first, I need to know its exact chemical mechanism.” Action: The LLM autonomously decides to trigger an external Tool. It formulates an API call: Execute: PubMed_Search(“Mechanism of action for Drug X”). Observation: The system executes the API call, retrieves the live data, and feeds it back into the LLM’s context window. Repeat: The LLM evaluates the observation. “Okay, I have the mechanism. Now I will take another action to search ClinicalTrials.gov for recent adverse events linked to this mechanism.”
This loop continues until the agent has synthesized a complete, comprehensive, and up-to-date answer.
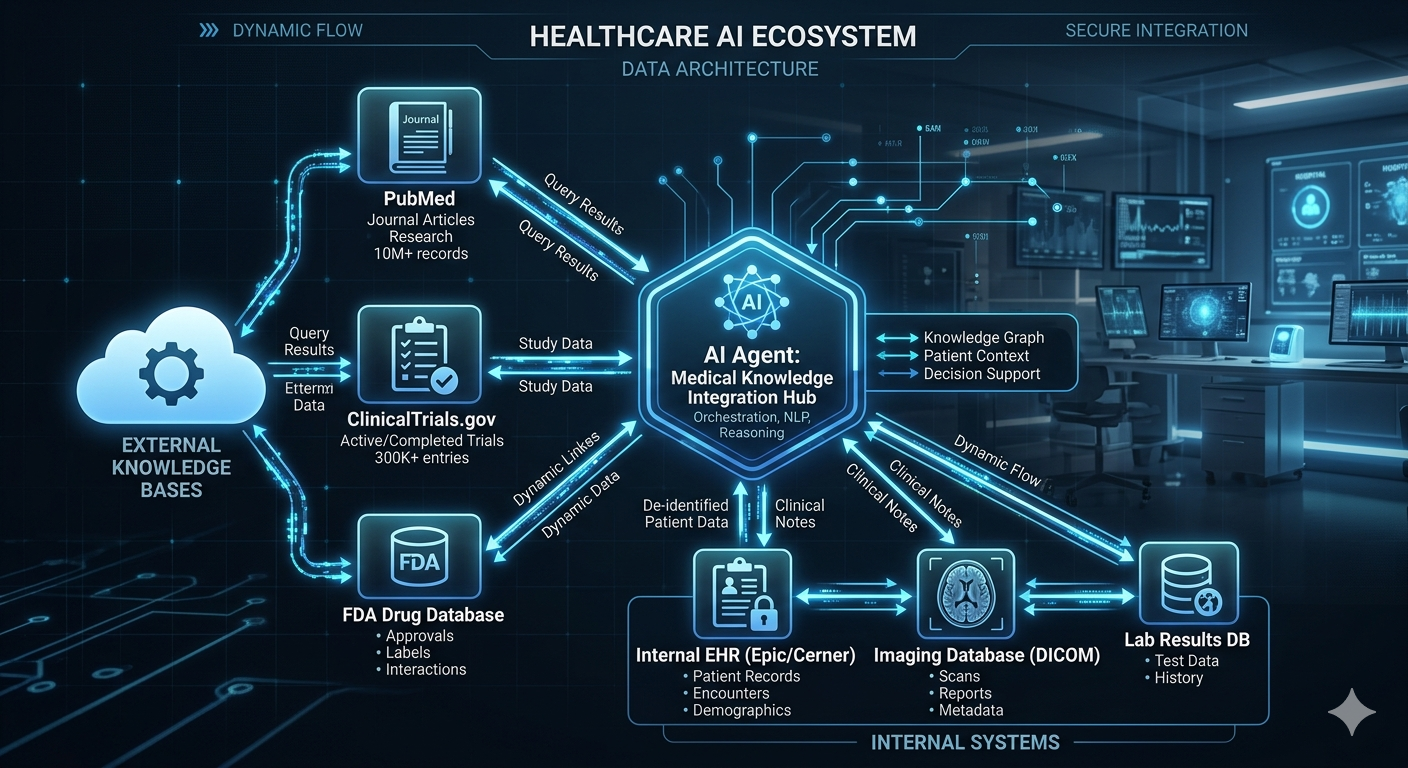
Equipping the Agent: The Clinical Toolkit An AI Agent is only as powerful as the tools it is given access to. When architecting these systems for MedTech clients, we design bespoke, secure toolkits that the LLM can trigger dynamically.
Example of a high-value clinical agent toolkit typically includes:
The Literature Tool: Live API access to PubMed, Arxiv, and medical journals. The agent can fetch abstracts, read full texts, and summarize findings in real-time. The Calculator Tool: LLMs are notoriously bad at math. By giving the agent a secure Python REPL (Read-Eval-Print Loop) tool, if it needs to calculate a patient dosage based on BMI or determine statistical significance, it writes the Python code, executes it, and reads the definitive mathematical output. The Internal EHR/Database Tool: Secure, sanitized read-only access to proprietary, anonymized patient data or internal surgical telemetry databases, allowing the agent to cross-reference public literature with internal historical outcomes.
Case Study: Real-World Impact: The ROI of Autonomy In a recent engagement with a leading surgical intelligence firm, we needed to bridge the gap between static pre-operative data and dynamic surgical planning.
We deployed an agentic architecture that didn’t just read data; it actively orchestrated workflows. When a surgeon queried a complex pre-op anatomical model, the agent didn’t just return a summary. It autonomously cross-referenced the specific patient’s anomaly against a database of similar historical surgeries, calculated the optimal entry angles using a geometric tool, and synthesized a multi-step surgical approach report.
The business outcome was twofold: First, it drastically reduced pre-operative planning time. Second, and more importantly for the executives, it standardized the quality of surgical insights across the entire department, regardless of an individual surgeon’s tenure.
Security, Compliance, and the Human-in-the-Loop Deploying autonomous agents in healthcare naturally raises compliance alarms. Will the agent go rogue? Will it access PHI (Protected Health Information)?
This is where Elite Technical Architecture separates itself from amateur coding.
We design these systems with strict deterministic guardrails. The agent operates within a secure VPC (Virtual Private Cloud). The “Tools” it has access to are heavily restricted via IAM (Identity and Access Management) roles.
Furthermore, we design Human-in-the-Loop (HITL) fail-safes. If the agent calculates a confidence score below a certain threshold, or if a multi-step plan involves a critical diagnostic recommendation, the architecture pauses the ReAct loop and pings a human specialist for authorization before proceeding.
You maintain the speed of autonomy with the safety of human clinical oversight.
Architecting these systems requires a rigorous approach to security and tool integration. I have documented this methodology in a 1-page Architectural Framework for ‘Deploying Autonomous AI Agents in Clinical R&D’.
Comment “BLUEPRINT” on my LinkedIn post, and I will DM it to you directly.
Conclusion:
The era of the LLM as a novelty chatbot is over. The era of the LLM as a deployable, scalable, and autonomous digital workforce has begun.
If your organization is spending premium capital on manual medical research, data extraction, or protocol synthesis, you have an architectural bottleneck that AI agents can solve today.