The surgical intervention is only the beginning of the patient’s journey. In orthopedics and sports medicine, a flawless glenoid joint replacement means very little if the patient fails to regain their full Range of Motion (ROM) during post-operative rehabilitation.
Historically, the MedTech industry has heavily invested in intra-operative precision while leaving post-operative monitoring in the dark ages. Today, patient recovery is largely assessed through infrequent clinic visits, reliant on subjective visual estimations or manual goniometers (physical protractors) applied by overworked physiotherapists.
This lack of objective, quantifiable, continuous data leads to delayed interventions, suboptimal recovery timelines, and poor data quality for longitudinal clinical trials.
We must close this gap. We must digitize human kinetics.
The Architectural Evolution: Markerless Pose Estimation Historically, achieving millimeter-accurate kinematic tracking required a dedicated biomechanics lab equipped with expensive Vicon optical systems and patients covered in reflective markers. This is unscalable for at-home telehealth.
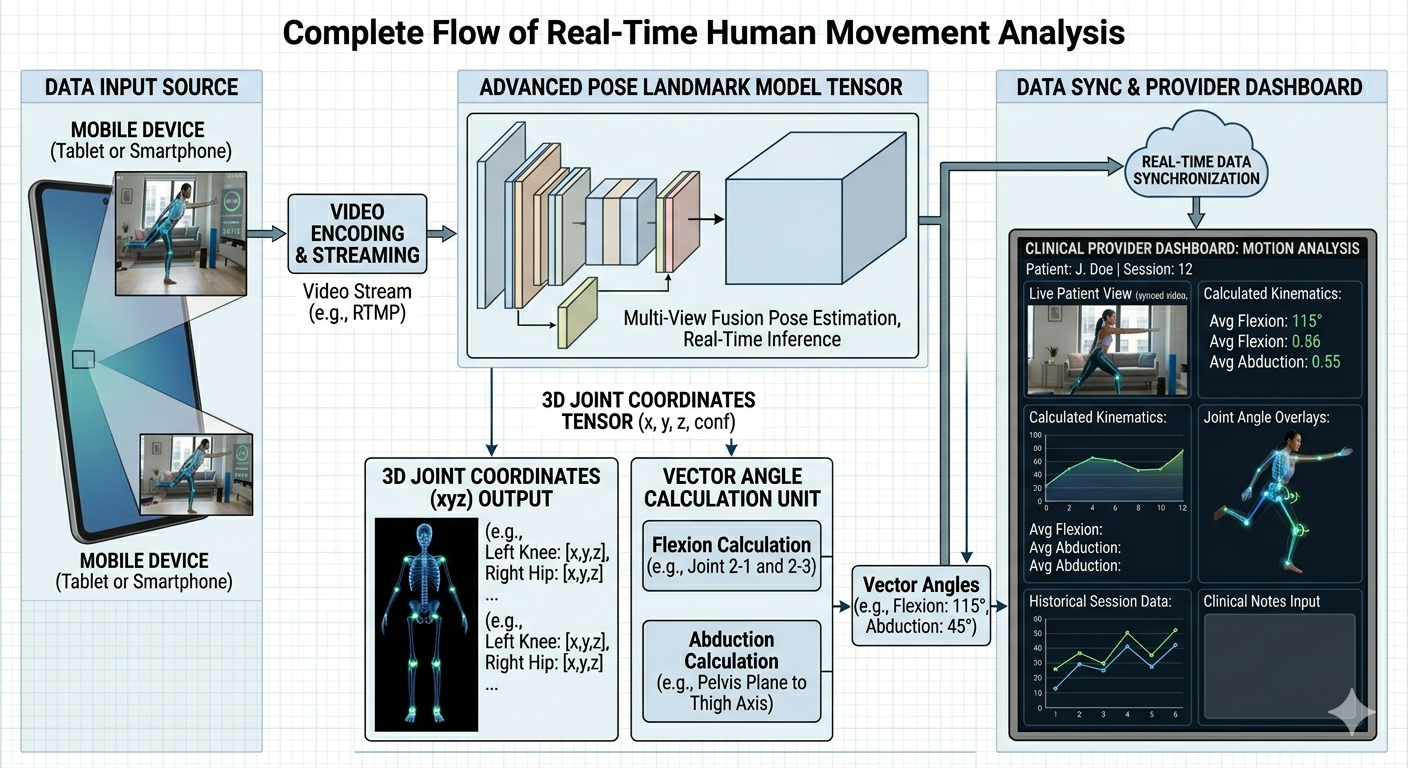
The architectural breakthrough lies in Markerless 3D Pose Estimation utilizing standard 2D RGB cameras (the smartphones and tablets your patients already own).
By leveraging highly optimized, edge-deployable deep learning frameworks (such as Google’s MediaPipe BlazePose topology), we can instantly infer the 3D spatial coordinates of 33 human body landmarks in real-time.
Case Study: Architecting the Digital ROM System In a recent architectural engagement with a premier surgical technology company, the mandate was clear: Empower physiotherapists with objective, quantifiable data to monitor shoulder and joint recovery protocols remotely.
To achieve this, we couldn’t just output a “stick figure.” We had to translate raw pixel data into actionable medical parameters.
The Architecture:
See content credentials Article content The Processing Engine: We embedded a cross-platform (iOS/Android) computer vision pipeline directly within a Unity engine framework. This provided the required graphical performance and sensor integration without relying on cloud-compute, ensuring zero-latency feedback for the patient. Kinematic Translation Layer: We wrote complex vector-math algorithms to translate the raw (x, y, z) spatial coordinates of the tracked landmarks into specific clinical metrics. Clinical Output: By analyzing the spatial vectors between the shoulder, elbow, and wrist nodes, the system autonomously calculated specific joint Flexion, Abduction, and Rotation angles in real-time.
The Business Outcome: This architecture fundamentally transformed the rehabilitation workflow. It replaced subjective guesswork with an evidence-based metric stream. Physiotherapists could now monitor patient compliance and physical progression daily via a clinical dashboard, allowing them to personalize therapy proactively and drastically accelerate the recovery timeline.
Solving the Depth Ambiguity Problem When architecting these systems, the primary technical hurdle is “Z-axis ambiguity.” A standard camera only sees in 2D. How does the AI know if a hand is moving up or moving forward towards the lens?
Elite architecture solves this through temporal tracking and kinematic constraints. The neural network doesn’t just look at a single frame; it tracks the temporal flow of the joints over time, applying physical constraints (e.g., an elbow cannot bend backward) to infer the correct 3D depth.
When you deploy this architecture correctly, the patient’s smartphone becomes a clinical-grade diagnostic sensor.